Venous thromboembolism (VTE), consisting of deep-vein thrombosis or pulmonary embolism, is a common yet underrecognized complication of cancer.1 VTE in patients with cancer accounts for approximately 20% of all VTE events in the United States.2 The diagnosis of cancer increases VTE risk by more than 4-fold, and VTE is the second leading cause of death in patients with cancer.1,2
Table 1 summarizes VTE risk factors in patients with cancer, including patient characteristics, tumor types, treatments, and biomarkers.2-6 The Khorana risk score (KRS) has emerged as a VTE risk stratification tool in ambulatory patients with cancer, accounting for body mass index, hemoglobin level, and/or use of erythropoiesis-stimulating agents, leukocyte count, platelet count, and tumor site.7 Although KRS has been validated in more than 15,000 patients with cancer with a variety of tumors, some data suggest that it is not predictive in specific cancers, such as lung cancer.7-9

The goal of this article was to review the management of VTE in patients with cancer, including prophylaxis and treatment, based on recently published randomized clinical trials, with a focus on the use of direct oral anticoagulants (DOACs).
Multiple oncology guidelines recommend against routine thromboprophylaxis in ambulatory patients with cancer.10-14 The American Society of Clinical Oncology (ASCO), European Society for Medical Oncology (ESMO), National Comprehensive Cancer Network (NCCN), and American Society of Hematology (ASH) guidelines include anticoagulation recommendations for hospitalized or perisurgical patients, with low-molecular-weight heparin (LMWH) as the most preferred option.10-14
The 2016 CHEST guidelines from the American College of Chest Physicians (ACCP) do not make recommendations for VTE prophylaxis in patients with cancer, but do recommend the use of LMWH over rivaroxaban, apixaban, edoxaban, or warfarin for the treatment of VTE in this patient population.14 However, these guidelines were published before the publication of recent DOAC clinical trials.14
The guidelines from ASCO, ASH, ESMO, and NCCN recommend VTE prophylaxis in patients with multiple myeloma who are receiving immunomodulatory agents and specify that VTE prophylaxis may be considered in “high-risk” patients; however, the definition of “high risk” is not clearly established in those guidelines.10-15
Clinical Trials on VTE Prophylaxis
Few studies have investigated the impact of VTE prophylaxis in ambulatory patients with cancer (Table 2).16-20 The PROTECHT and SAVE-ONCO clinical trials demonstrated statistically significant reductions in VTE incidence with LMWH as primary prevention in ambulatory patients with cancer (Table 2).16,17 In the PROTECHT study, most subgroups showed lower rates of VTE with the use of nadroparin compared with placebo, except for the pancreatic cancer group.16 The SAVE-ONCO study stratified VTE by cancer type, stage, and baseline risk.17 In neither trial did the investigators use a risk assessment tool for enrollment.
Although the primary end points in PROTECHT and SAVE-ONCO met their statistical threshold,16,17 the results did not radically change prescribing practices or prompt clinical practice guideline updates, given the low magnitude of VTE reduction. Based on a low benefit–risk profile, the guidelines for VTE prophylaxis did not change.

Two recent trials evaluated use of DOACs to prevent VTE in high-risk, ambulatory patients with cancer. The AVERT clinical trial investigated the use of apixaban for VTE prevention, whereas the CASSINI clinical trial investigated rivaroxaban in a similar setting (Table 2).17,18 Both studies required KRS of ≥2 to target patients at high risk for VTE. Although both studies showed efficacy in preventing VTE, the differences in study design, population, and screening were notable.18,19
The CASSINI study enrolled a large number of patients with pancreatic and gastric cancers, both known to pose a very high VTE risk compared with the AVERT study, which had an increased rate of gynecologic cancers and lymphoma.18,19 CASSINI excluded 4.5% (N = 49) of patients presenting with baseline asymptomatic VTE, having relatively stringent inclusion criteria, but that did not reflect a real-world population, because baseline ultrasound screening is not done routinely in clinical practice.19 Patients in the AVERT study did not undergo baseline ultrasound screening.18
Screening differences between the 2 studies highlight the potential for variance in primary outcomes, potentially resulting in lower overall event rates in the CASSINI study.19 Patients in the AVERT study might have received benefit from apixaban for the treatment of an asymptomatic VTE that was present at baseline.18
AVERT demonstrated a statistically significant difference in the primary outcome of VTE reduction in the modified intention-to-treat population, or in all randomized patients who received at least 1 dose of the study drug.18 CASSINI did not show a significant difference in the primary outcome of VTE reduction in the intention-to-treat population, which included all randomized patients, regardless of drug administration.19 Notably, a statistically significant reduction in VTE was found in the prespecified treated population in CASSINI.19 Both studies had high discontinuation rates—37% in the AVERT study and 47% in the CASSINI study. Nearly 40% of events in CASSINI were in patients after treatment discontinuation. Adverse events did not contribute to discontinuation and were not different between the placebo versus the active treatment groups.18,19
One prospective pilot study evaluated the use of apixaban 2.5 mg twice daily for 6 months in patients with multiple myeloma who received first-line thalidomide-based treatment or second-line lenalidomide-based treatment.19 Among the 104 patients, 2 venous thrombotic events were registered. In all, 1 major and 11 clinically relevant nonmajor bleeding events were reported, demonstrating that apixaban may be effective and safe in preventing VTE in patients with multiple myeloma who receive treatment with immunomodulatory drugs.21
Currently, 2 randomized clinical trials, one with rivaroxaban versus aspirin (NCT03428373) and one with apixaban versus placebo (NCT02958969), are underway.22,23
Venous Thromboembolism Treatment Trials
Although DOACs are not recommended for use as routine primary VTE prophylaxis in all patients with cancer, they are emerging for use for VTE treatment or to reduce VTE recurrence.2 Table 3 summarizes major clinical trials with DOACs used for VTE treatment.24-26
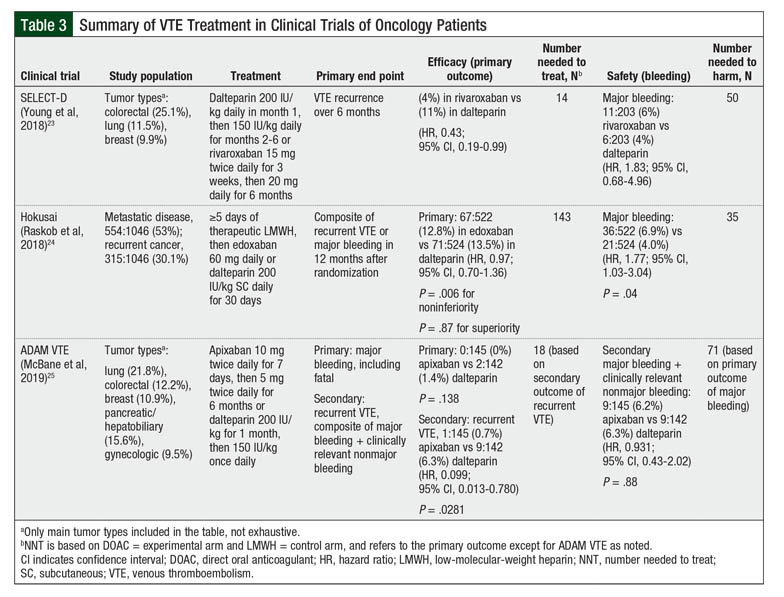
The SELECT-D clinical trial demonstrated a decreased rate of recurrent VTE with rivaroxaban compared with dalteparin (4% vs 11%, respectively; hazard ratio [HR], 0.43; 95% confidence interval [CI], 0.19-0.99), but an increase in clinically relevant nonmajor bleeding events (HR, 3.76; 95% CI, 1.63-8.69).24 Based on the results from this study, the updated 2020 NCCN clinical guidelines include rivaroxaban as an option for VTE treatment for patients with cancer.12,24
Similarly, the Hokusai VTE Cancer clinical trial determined that edoxaban was noninferior to dalteparin with respect to a composite end point of recurrent VTE or major bleeding (edoxaban, 12.8% vs dalteparin, 13.5%; HR, 0.97; 95% CI, 0.70-1.36).25 Edoxaban had lower VTE recurrence rates but higher rates of bleeding.25 Edoxaban is now also included as an option for the treatment of VTE in the NCCN guidelines after the completion of at least 5 days of LMWH or unfractionated heparin therapy.12
The investigator-initiated ADAM VTE clinical trial identified lower rates of recurrent VTE with apixaban versus dalteparin (0.7% vs 6.3%, respectively; HR, 0.099; 95% CI, 0.013-0.780; P = .0281), and lower bleeding rates were noted in the apixaban group (apixaban 0% vs dalteparin 1.4%; P = .138).26 Based on these study results, apixaban is included in the NCCN guidelines as a second-line option for VTE treatment for patients who refuse or are intolerant of treatment with LMWH.15,26
Clinical Considerations
In light of these recent clinical trials supporting the use of DOAC for VTE prophylaxis and treatment, the updated ASCO 2019 guidelines include the use of rivaroxaban and apixaban as thromboprophylaxis options for patients at high risk for VTE, as well as the addition of rivaroxaban and edoxaban as VTE treatment options.10 Specifically, the use of DOAC is mentioned as a prophylaxis option for those at high risk, which is defined by a pretreatment KRS of ≥2.10
Utilizing KRS screening or incorporating a system with frequent monitoring for VTE symptoms may be warranted, given the high risk for VTE in the ambulatory oncology setting. For example, one study showed a high rate (8.5%) of baseline asymptomatic VTE in patients with a KRS of ≥3, suggesting that upfront ultrasonography may be beneficial in very high-risk patients.27
ASCO was the first organization to incorporate DOACs into its guideline recommendations and to consider those agents for upfront thromboprophylaxis in high-risk outpatients.10 The NCCN guidelines were also updated to include apixaban and rivaroxaban as VTE prophylaxis options in intermediate- or high-risk patients based on KRS of ≥2, and added apixaban, edoxaban, and rivaroxaban as VTE treatment options for oncology patients.12 We expect that other organizations may follow suit.
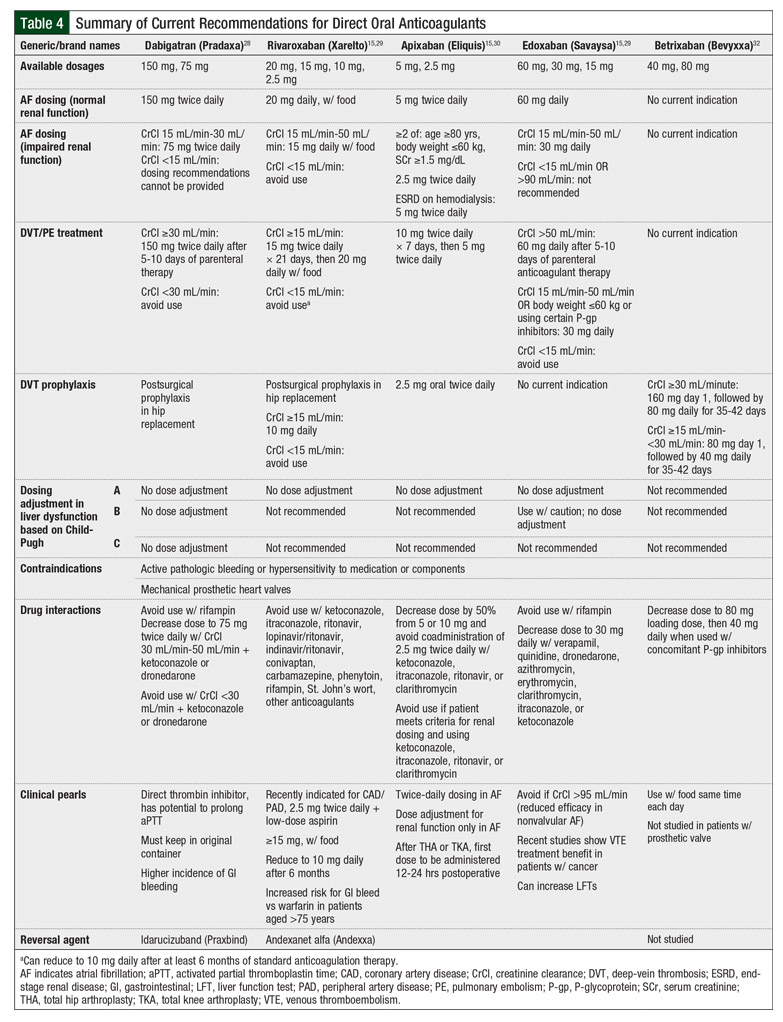
Although DOACs offer a more convenient administration method than the daily injections required with LMWH, the decision to use DOACs should involve the evaluation of patient-specific factors, such as renal and hepatic function, drug interactions, insurance coverage, and bleeding risk (particularly in those with gastrointestinal cancers).
Table 4 provides summaries of important information about DOACs regarding dosing, contraindications, drug interactions, and other clinical pearls that are highly relevant to pharmacy practice.12,28-32 Of the DOACs studied for VTE prophylaxis in ambulatory patients with cancer, only rivaroxaban should be avoided in the setting of renal impairment, when the creatinine clearance decreases to ≤15 mL/min.28-32 The prescribing information for apixaban and for rivaroxaban suggest that strong inhibitors or inducers of P-glycoprotein or cytochrome P3A4 can increase or decrease drug concentrations and potentially alter the safety and efficacy of these drugs.29,30
Whereas KRS was used in the AVERT and the CASSINI studies, no standard guideline recommendation exists for KRS screening frequency, timing, or appropriateness for specific tumor types.18,19 Although some experts believe that KRS may be improved as a risk stratification tool by incorporating performance status, biomarker measurements, and chemotherapy type,7,33 KRS continues to be widely recognized as a user-friendly and simple screening modality.34
The major limitations of KRS include the requirement for multiple laboratory parameters and inclusion of specific tumor types.7 KRS does not include hematologic malignancies and does not utilize other validated markers, such as D-dimer or clinical factors such as history of VTE. Other tools are scores used in the CONKO, PROTECHT, and the Vienna Cancer and Thrombosis Study (CATS).6,35-37
In a comparative analysis, the PROTECHT16,36 and the Vienna CATS scores35 demonstrated better efficacy in discerning between high- and low-risk patients than the KRS tool.6 D-dimer results from the Vienna CATS35 and the use of gemcitabine or platinum-based chemotherapy from the PROTECHT study16,36 were significantly associated with VTE risk.6
Creating a standardized tool that is applicable across all disease states and treatments may be beneficial to identify high-risk patients who could benefit from VTE prophylaxis. The ideal tool would strike the right balance between predictive utility and complexity or ease of use in practice. Embedding KRS or another risk stratification tool in the electronic medical record may help to trigger high-risk patients who would benefit from referral to a nonmalignant hematology specialist for consideration of screening ultrasonography or thromboprophylaxis.
Considering that KRS may not perform optimally in all tumor types, particularly in hematologic malignancies and even in some solid tumors, such as lung,8 a call for tumor-specific studies is warranted. A prospective trial comparing the use of gemcitabine with or without dalteparin in patients with pancreatic cancer demonstrated no fatal VTE in the dalteparin group compared with 5 (8.3%) of 62 patients in the gemcitabine-only group (P = .057), which suggests that upfront initiation of VTE prophylaxis in pancreatic cancer may impact VTE-related mortality rates.20 This study also noted reduced VTE with dalteparin, from 23% to 3.4%.30 Fewer studies exist across other solid tumors or hematologic malignancies.
VTE treatment studies comparing LMWH with DOACs demonstrated that DOACs are at least noninferior to LMWH, if not more effective, but may be associated with increased bleeding risk.24-26,38 Based on these data, DOACs are likely to be noninferior to LMWH for VTE prophylaxis, although it is unlikely that large randomized clinical trials will be conducted to confirm this.
As noted earlier, randomized clinical trials are ongoing to understand better the risk–benefit profile of administering DOACs in patients with multiple myeloma. This is especially the case when considering that aspirin prophylaxis alone is not sufficient to reduce VTE risk in most patients with multiple myeloma, along with the trend toward greater patient preference for DOACs versus LMWH.39,40
Conclusion
Further research should optimize and standardize VTE risk stratification tools for clinical implementation, striking the right balance between drug efficacy and safety. The decision for thromboprophylaxis may also differ based on the timing of the cancer diagnosis, the treatment, and the tumor type. Nonetheless, a concerted effort should be made by all health professionals caring for patients with cancer to screen for VTE risk using available tools, such as KRS, as well as to consider appropriate interventions, including patient counseling on signs and symptoms of VTE, referral to a nonmalignant hematology specialist, screening ultrasound for baseline VTE, or thromboprophylaxis.
Author Disclosure Statement
Dr Hanson and Dr Maher have no conflicts of interest to report. Dr Patel is a Consultant to and has received research support/honoraria from Janssen Research & Development.
References
- Imberti D, Agnelli G, Ageno W, et al. Clinical characteristics and management of cancer-associated acute venous thromboembolism: findings from the MASTER Registry. Haematologica. 2008;93:273-278.
- Karimi M, Cohan N. Cancer-associated thrombosis. Open Cardiovasc Med J. 2010;4:78-82.
- Kraaijpoel N, Carrier M. How I treat cancer-associated venous thromboembolism. Blood. 2019;133:291-298.
- Heit JA, O’Fallon WM, Petterson TM, et al. Relative impact of risk factors for deep vein thrombosis and pulmonary embolism: a population-based study. Arch Intern Med. 2002;162:1245-1248.
- Wun T, White RH. Venous thromboembolism (VTE) in patients with cancer: epidemiology and risk factors. Cancer Invest. 2009;27(Suppl 1):63-74.
- van Es N, Di Nisio M, Cesarman G, et al. Comparison of risk prediction scores for venous thromboembolism in cancer patients: a prospective cohort study. Haematologica. 2017;102:1494-1501.
- Khorana AA, Kuderer NM, Culakova E, et al. Development and validation of a predictive model for chemotherapy-associated thrombosis. Blood. 2008;111:4902-4907.
- Mansfield AS, Tafur AJ, Wang CE, et al. Predictors of active cancer thromboembolic outcomes: validation of the Khorana score among patients with lung cancer. J Thromb Haemost. 2016;14:1773-1778.
- Angelini D, Khorana AA. Risk assessment scores for cancer-associated venous thromboembolic disease. Semin Thromb Hemost. 2017;43:469-478.
- Key NS, Khorana AA, Kuderer NM, et al. Venous thromboembolism prophylaxis and treatment in patients with cancer: ASCO clinical practice guideline update. J Clin Oncol. 2020;38:496-520.
- Mandalà M, Falanga A, Roila F, for the ESMO Guidelines Working Group. Management of venous thromboembolism (VTE) in cancer patients: ESMO Clinical Practice Guidelines. Ann Oncol. 2011;22(Suppl 6):vi85-vi92.
- Streiff MB, Holmstrom B, Angelini D, et al. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines), Cancer-Associated Venous Thromboembolic Disease. Version 1.2020. April 16, 2020. www.nccn.org/professionals/physician_gls/pdf/vte.pdf. Accessed May 1, 2020.
- Cuker A, Arepally GM, Chong BH, et al. American Society of Hematology 2018 guidelines for management of venous thromboembolism: heparin-induced thrombocytopenia. Blood Adv. 2018;2:3360-3392.
- Kearon C, Akl EA, Ornelas J, et al. Antithrombotic therapy for VTE disease: CHEST guideline and expert panel report. Chest. 2016;149:315-352.
- Palumbo A, Rajkumar SV, Dimopoulos MA, et al. Prevention of thalidomide- and lenalidomide-associated thrombosis in myeloma. Leukemia. 2008;22:414-423.
- Agnelli G, Gussoni G, Bianchini C, et al, for the PROTECHT Investigators. Nadroparin for the prevention of thromboembolic events in ambulatory patients with metastatic or locally advanced solid cancer receiving chemotherapy: a randomised, placebo-controlled, double-blind study. Lancet Oncol. 2009;10:943-949.
- Agnelli G, George DJ, Kakkar AK, et al. Semuloparin for thromboprophylaxis in patients receiving chemotherapy for cancer. N Engl J Med. 2012;366:601-609.
- Carrier M, Abou-Nassar K, Mallick R, et al. Apixaban to prevent venous thromboembolism in patients with cancer. N Engl J Med. 2019;380:711-719.
- Khorana AA, Soff GA, Kakkar AK, et al. Rivaroxaban for thromboprophylaxis in high-risk ambulatory patients with cancer. N Engl J Med. 2019;380:720-728.
- Maraveyas A, Waters J, Roy R, et al. Gemcitabine versus gemcitabine plus dalteparin thromboprophylaxis in pancreatic cancer. Eur J Cancer. 2012;48:1283-1292.
- Pegourie B, Karlin L, Benboubker L, et al; IFM Group. Apixaban for the prevention of thromboembolism in immunomodulatory-treated myeloma patients: Myelaxat, a phase 2 pilot study. Am J Hematol. 2019;94:635-640.
- Lawson Health Research Institute. ASA vs. rivaroxaban in newly diagnosed or relapsed and refractory multiple myeloma patients treated with len-dex combination. https://clinicaltrials.gov/ct2/show/NCT03428373. NLM Identifier: NCT03428373. Accessed March 12, 2020.
- Piazza G. Apixaban for primary prevention of venous thromboembolism in patients with multiple myeloma. https://clinicaltrials.gov/ct2/show/NCT02958969. NLM Identifier: NCT02958969. Accessed March 12, 2020.
- Young AM, Marshall A, Thirlwall J, et al. Comparison of an oral factor Xa inhibitor with low molecular weight heparin in patients with cancer with venous thromboembolism: results of a randomized trial (SELECT-D). J Clin Oncol. 2018;36:2017-2023.
- Raskob GE, van Es N, Verhamme P, et al for the Hokusai VTE Cancer Investigators. Edoxaban for the treatment of cancer-associated venous thromboembolism. N Engl J Med. 2018;378:615-624.
- McBane RD 2nd, Wysokinski WE, Le-Rademacher JG, et al. Apixaban and dalteparin in active malignancy-associated venous thromboembolism: the ADAM VTE trial. J Thromb Haemost. 2020;18:411-421.
- Khorana AA, Francis CW, Kuderer NM, et al. Dalteparin thromboprophylaxis in cancer patients at high risk for VTE: a randomized trial. Thromb Res. 2017;151:89-95.
- Pradaxa (dabigatran etexilate mesylate) capsules, for oral use [prescribing information]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals; 2019.
- Xarelto (rivaroxaban) tablets, for oral use [prescribing information]. Titusville, NJ: Janssen Pharmaceuticals; 2020.
- Eliquis (apixaban) tablets, for oral use [prescribing information]. New York, NY: Pfizer; 2019.
- Savaysa (edoxaban) tablets for oral use [prescribing information]. Parsippany, NJ: Daiichi Sankyo; 2015.
- Bevyxxa (betrixaban) capsules, for oral use [prescribing information]. South San Francisco, CA: Portola Pharmaceuticals; 2017.
- Pabinger I, van Es N, Heinze G, et al. A clinical prediction model for cancer associated venous thromboembolism: a development and validation study in two independent prospective cohorts. Lancet Haematol. 2018;5:e289-e298. Epub 2018 Jun 7. doi.org/10.1016/S2352-3026(18)30063-2.
- Khorana AA. Simplicity versus complexity: an existential dilemma as risk tools evolve. Lancet Haematol. 2018;5:e273-e274. Epub 2018 Jun 7. doi.org/10.1016/S2352-3026(18)30067-X.
- Simanek R, Vormittag R, Ay C, et al. High platelet count associated with venous thromboembolism in cancer patients: results from the Vienna Cancer and Thrombosis Study (CATS). J Thromb Haemost. 2010;8:114-120.
- Verso M, Agnelli G, Barni S, et al. A modified Khorana risk assessment score for venous thromboembolism in cancer patients receiving chemotherapy: the Protecht score. Intern Emerg Med. 2012;7:291-292.
- Pelzer U, Sinn M, Stieler J, Riess H. Primary pharmacological prevention of thromboembolic events in ambulatory patients with advanced pancreatic cancer treated with chemotherapy? [in German]. Dtsch Med Wochenschr. 2013;138:2084-2088.
- Li A, Garcia DA, Lyman GH, Carrier M. Direct oral anticoagulant (DOAC) versus low-molecular-weight heparin (LMWH) for treatment of cancer associated thrombosis (CAT): a systematic review and meta-analysis. Thromb Res. 2019;173:158-163.
- Hutchinson A, Rees S, Young A, et al. Oral anticoagulation is preferable to injected, but only if it is safe and effective: an interview study of patient and carer experience of oral and injected anticoagulant therapy for cancer-associated thrombosis in the SELECT-D trial. Palliat Med. 2019;33:510-517.
- Sanfilippo KM, Luo S, Carson KR, et al. Aspirin may be inadequate thromboprophylaxis in multiple myeloma. Blood. 2017;130(Suppl 1):3419.