Symptom Overview
Vancomycin infusion reaction (VIR), also referred to as vancomycin flushing syndrome and formerly known as “red man syndrome,” is an infusion-related anaphylactoid reaction that is peculiar to the glycopeptide antibiotic vancomycin.1 VIR often occurs after the rapid infusion of the first dose of vancomycin, but VIR-like reaction can similarly be caused by treatment with other intravenous (IV) antibiotics (including ciprofloxacin, amphotericin B, and rifampicin), or other drugs that stimulate histamine release.1
This review article will elucidate the clinical practice guidelines for the effective, evidence-based management of VIR, with a particular focus on vancomycin hypersensitivity, and will include an overview of the symptomatic presentation of VIR and a discussion of its epidemiology and etiology. This review will conclude with a general overview of the main treatment options available for VIR and a discussion of other relevant therapeutic considerations for VIR.
VIR is the most common hypersensitivity reaction associated with vancomycin use.1 The incidence of VIR is estimated to be 3.7% to 47% in patients who receive treatment with IV vancomycin.2 An investigation into the incidence of VIR in healthy volunteers showed that 30% to 90% of those who received vancomycin had VIR1 (the original source: Ross M. Red-man syndrome: a preventable adverse drug reaction. www.vh.org/Providers/Publications/PTNews/993/12.93.html, is no longer accessible). VIR is often mild and easily treated, but it has the potential to cause severe adverse reactions in some individuals.1 Although rare, such adverse events are more frequent in individuals aged <40 years.3
The presence of VIR in a patient receiving an infusion of vancomycin can be identified by a characteristic cluster of symptoms.4 The symptoms that fall under the umbrella of VIR include flushing, pruritus, chest pain, muscle spasm, and hypotension.4 Although flushing and pruritus are the most common symptoms of VIR, patients may also have these 2 symptoms in conjunction with the other symptoms listed above.4
In a series of clinical case reports, adverse reactions typically occurred within 15 to 45 minutes of starting an infusion of vancomycin and persisted throughout the duration of the infusion.4 The symptoms typically resolved within 30 minutes after ending the infusion, and in some situations, symptom resolution began as the infusion neared completion.4 Patient variability is a strong factor in the severity and recurrence of VIR, and patients may present with varying intensities of the symptoms.4
Etiology
The cause of VIR is most often attributed to the direct degranulation of mast cells and basophils by vancomycin. This degranulation results in the release of histamine independent of an immunoglobulin (Ig)E-mediated or complement-mediated mechanism, and is occurring without evidence of the involvement of other antibodies (ie, IgG) or immune complexes.1 Thus, the hypersensitivity reaction that underlies VIR is characteristically anaphylactoid (ie, nonimmunologic anaphylaxis).1
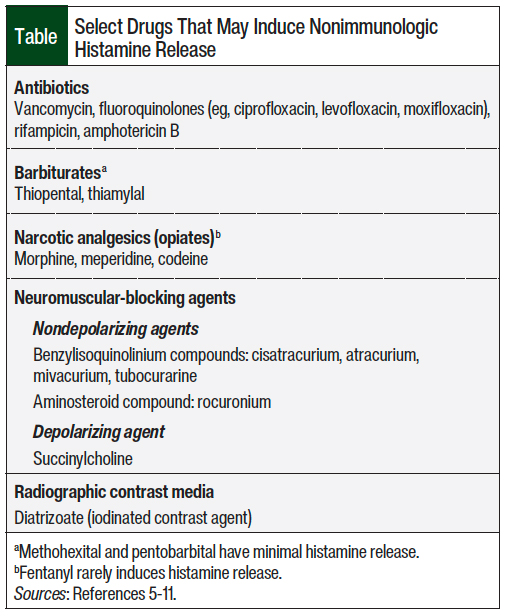
As noted earlier, several other drugs can cause nonimmunologic histamine release that can predispose patients to VIR and/or prevent the successful desensitization to vancomycin (Table).5-11
On mast-cell and basophil stimulation, the release of histamine causes the associated symptoms of flushing, pruritus, chest pain, muscle spasm, and hypotension.1,12 VIR occurs most frequently after the use of IV vancomycin; however, cases of VIR after the oral and intraperitoneal administrations of vancomycin have been reported.1,12
The manifestation of VIR after oral vancomycin administration has been reported in patients with Clostridium difficile infection.13 In these individuals, inflammation of the gastrointestinal tract is believed to bolster the otherwise poor enteral absorption of vancomycin.13
The increased systemic absorption of oral vancomycin and the risk for a hypersensitivity reaction have been associated with several other factors, including vancomycin administration of 10 days or more or dosages of more than 500 mg/day, history of other hypersensitivities or cystic fibrosis, and renal dysfunction.14 However, a few published case reports have also observed VIR in patients with normal renal function,15-18 although additional studies are still needed to further substantiate these observations. For most cases, discontinuation of oral vancomycin and the administration of an antihistamine, such as diphenhydramine, were sufficient to resolve VIR.13
The rate of vancomycin infusion is an important factor in VIR: more rapid infusion (1 g in <1 hour) is associated with a higher incidence of VIR than the slower infusion of vancomycin.1,12 The signs and symptoms of VIR can begin to manifest 4 to 10 minutes after the start of vancomycin administration, and some symptoms have even occurred shortly after the infusion had stopped.1,12
Delayed VIR has been reported in patients receiving therapy for longer than 7 days after a 90- to 120-minute infusion of vancomycin.1 The severity of VIR can vary with multiple exposures to vancomycin and can still manifest with slower infusions, albeit with less frequency than with shorter and faster exposures to vancomycin.1
The Approach to Management
VIR is often self-limiting or may progress to an acute condition that requires medical intervention, depending on the severity of the patient’s reaction, the severity of the infection, or the patient’s overall health. This can be determined using qualitative and quantitative clinical scoring systems, such as patient-reported outcomes evaluating the subjective severity of pruritus and the percentage of total body surface area to determine the extent of erythema, respectively.19
In general, acute VIR can be characterized by 3 levels of severity, including mild reactions, in which the patient can tolerate flushing and other symptoms; moderate reactions, in which the patient is uncomfortable as a result of flushing or pruritus, is hemodynamically stable, and does not have chest pain or muscle spasms; and severe reactions, in which the patient has muscle spasms, chest pain, and/or hypotension.5
The efficacy of pretreatment with antihistamines in reducing the incidence and severity of VIR was evaluated in several studies, reporting that pretreatment with oral or IV histamine type 1 (H1) antagonists (eg, hydroxyzine or diphenhydramine ≤1 mg/kg) and/or histamine type 2 (H2) antagonists (eg, cimetidine ≤4 mg/kg) 1 hour before dosing vancomycin could attenuate the effects from rapid vancomycin administration (infusions rate ≤10 mg/min), often required in emergency or presurgical setting4,5,20,21; however, careful monitoring of patients during subsequent doses is still necessary. When VIR is moderate or severe, multiple studies have also shown that the use of oral antihistamines that target the H1 and H2 receptors is successful in reducing the severity of VIR symptoms.4,5,20,21
After the vancomycin infusion is stopped for moderate-to-severe VIR, clinical guidelines suggest 50-mg diphenhydramine (oral or IV) and 20-mg IV famotidine be introduced.5 IV fluids may also be used to achieve hemodynamic stabilization if the patient is hypotensive. The vancomycin infusion is then restarted at a reduced rate once the patient has returned to the prereaction clinical status.5
Specifically, the infusion rate can be reduced to 50% of the original rate or decreased to <1000 mg/hr, with a target of 10 mg/min, whichever is slower.5,22 Based on the results of their study, Healy and colleagues recommended increasing the duration of infusions to 2 hours for patients with VIR who are receiving 1-hour infusions, because trough concentrations and the areas under the curve with vancomycin were similar for the 1- and 2-hour infusions.23 A lower vancomycin dose, given in a more frequent schedule (eg, 500 mg every 6 hours instead of 1 g every 12 hours), can also help prevent VIR; however, there may be relevant pharmacokinetic, workflow, and financial implications to consider.4
Another recommended approach for the management of VIR in patients with a history of an adverse reaction is to avoid the use of vancomycin and opt for an alternative antibiotic with similar activity and efficacy to vancomycin. The main recommendation is to use the cyclic lipopeptide antibiotic daptomycin or the semisynthetic lipoglycopeptide antibiotics (and vancomycin analogs) telavancin, dalbavancin, and oritavancin.5
The standard doses for daptomycin range from 4 to 6 mg/kg once daily for skin and skin structure infections to 8 to 10 mg/kg once daily for bloodstream infections, for a duration of usually 5 to 14 days.24 By contrast, telavancin is usually dosed at 10 mg/kg once daily for ≥14 days for bloodstream infections, whereas the recommended doses for oritavancin and dalbavancin as long-acting antibiotics are 1.2 g and 1.5 g, respectively, as single doses for skin and soft-tissue infections.25-27
Although adverse events have been reported with the use of these lipoglycopeptide agents, including pseudoallergic VIR with dalbavancin and with oritavancin, these are limited and are less frequent than with vancomycin.5 With dalbavancin and oritavancin, pseudo-VIR symptoms can often be managed by using slower infusion rates.5
Outside of the United States, another alternative treatment to vancomycin is teicoplanin, which is a glycopeptide antibiotic that has an antibacterial spectrum similar to that of vancomycin.4 Treatment with teicoplanin results in fewer infusion-related reactions than vancomycin, so teicoplanin may be a safer alternative for patients who cannot tolerate vancomycin-induced release of histamine.4,21
The recommended loading dose for teicoplanin is 6 mg/kg twice daily for 48 hours for uncomplicated infections, followed by a maintenance dose of 6 mg/kg once daily, thereafter; complicated infections require the continuation of a high-dose regimen of teicoplanin.28 However, because teicoplanin is moderately expensive compared with vancomycin and is not widely available, alternative antibiotics, such as those discussed above, should be considered instead.
Although all of these antibiotic alternatives can be effectively used in place of vancomycin, it is still important that patients who have had VIR be actively monitored when using these agents, and that their specified indications, dosages, and side-effect profiles be carefully considered before proceeding with an antibiotic substitution.
The percentage of patients who require an alternative therapy for VIR is generally low, but considerable variability exists in this area, because rarer forms of vancomycin hypersensitivity, which can manifest as IgE-mediated (immunologic) anaphylaxis, drug-induced hypersensitivity syndrome, or linear IgA bullous dermatosis, may still necessitate such treatment.5
When considering alternative antibiotics for patients with a history of serious hypersensitivity reactions to vancomycin, it is often recommended that other treatment options besides related glycopeptide agents are explored beforehand, and used whenever possible.5
Appropriate precautions may also be taken before the use of an alternative antibiotic therapy is considered, including slowing the infusion rate and completing relevant premedication or coadministration of H1 and H2 antagonists. For patients with a history of anaphylaxis to vancomycin, alternative therapy with nonglycopeptide antibiotic is recommended whenever possible.5
If, however, vancomycin is the only effective antibiotic option available for a patient who has VIR with the first dose, then it is recommended that the second dose of vancomycin be given over ≥2 hours after pretreatment with an H1 antagonist (Figure).4,5,23,28
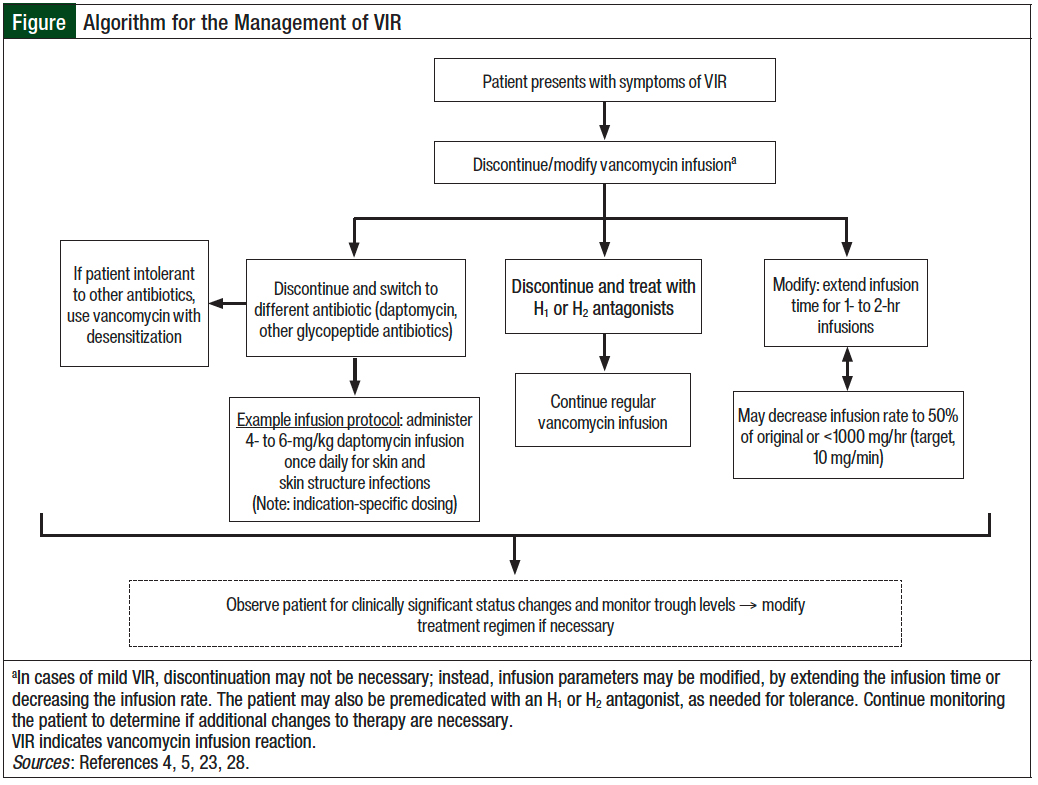
For patients with serious infections that cannot be adequately treated with alternative antibiotics, or for those with recurrent VIR despite premedication and slower infusion rates, vancomycin desensitization should be used (Figure). This is when vancomycin is gradually reintroduced to a patient by incrementally increasing the dose, to reach a state of temporary clinical tolerance, allowing the drug to be safely administered to the patient as long as the patient is continually exposed to it.5
Several desensitization protocols have been published, and indicate that the completion period ranges from several hours for rapid desensitization (indicated for acute cases) to several days for slow desensitization (when intermittent doses are incrementally increased for less severe cases).5,29-31
The symptoms during desensitization are usually mild, including limited urticaria, flushing, and pruritus, and can typically be managed without the complete discontinuation of the desensitization protocol, by briefly stopping the infusion and treating symptoms that do not subside spontaneously.5
Whenever vancomycin is used for treatment in an individual who is susceptible to VIR, it is necessary to observe the patient closely during the infusion, which should be promptly stopped if the patient has severe symptoms, including a clinically significant decrease in blood pressure, muscle spasms, respiratory distress, or any muscle or chest pains.4 Ultimately, the decision to proceed with desensitization depends on the patient’s status and the need for vancomycin treatment. Desensitization should only be considered if vancomycin is absolutely required, in cases where the patient displays an intolerance toward alternative antibiotics, or if no equally effective antibiotic is available.
After desensitization is initially completed, the patient can receive subsequent doses of vancomycin with no anticipated symptoms; patient observation is still necessary.5 Accordingly, it is important that serum levels of vancomycin be carefully monitored to prevent drug levels from dropping below detectable limits. If the drug level does become undetectable, then the desensitization protocol should be repeated for the safe reintroduction of the medication.5
It is also important that vancomycin be kept within the therapeutic range for infection treatment and to maintain drug tolerance, which can be achieved using continuous, rather than intermittent, infusions.5 In any case, after desensitization, the patient should be clearly told that he or she still has an allergy to vancomycin and may require desensitization again in the future.5
Conclusion
VIR is a common hypersensitivity reaction to vancomycin infusion that is well-documented in diverse patient populations. The best form of treatment remains slowing the vancomycin infusions to a target rate of ≤10 mg/min. Premedications may also be completed with H1 or H2 antagonists, as needed, or if more rapid infusions of vancomycin are required. Other treatment recommendations may include vancomycin desensitization or using alternative antibiotic therapy, specifically in patients who are predisposed to hypersensitivity reactions.
There are, however, various therapeutic considerations that must be made before deciding on a single treatment strategy. Clinicians should approach the treatment holistically and use these treatment recommendations in combination with other standard clinical practice guidelines to maximize the evidence-based care of patients with VIR.
Author Disclosure Statement
The authors have no conflicts of interest to report.
References
- Sivagnanam S, Deleu D. Red man syndrome. Crit Care. 2003;7:119-121.
- Wazny LD, Behnam D. Desensitization protocols for vancomycin hypersensitivity. Ann Pharmacother. 2001;35:1458-1464.
- Korman T, Turnidge J, Grayson M. Risk factors for cutaneous reactions associated with intravenous vancomycin. J Antimicrob Chemother. 1997;39:371-381.
- Wallace MR, Mascola JR, Oldfield EC III. Red man syndrome: incidence, etiology, and prophylaxis. J Infect Dis. 1991;164:1180-1185.
- Weller PF. Vancomycin hypersensitivity. UpToDate. Wolters Kluwer; 2021. www.uptodate.com/contents/vancomycin-hypersensitivity. Accessed September 13, 2021. [Subscription required to access.]
- Singh J, Daftary A. Iodinated contrast media and their adverse reactions. J Nucl Med Technol. 2008;36:69-74; quiz 76-77.
- Skibiski J. Barbiturates. StatPearls. February 9, 2021. www.statpearls.com/ArticleLibrary/viewarticle/18133. Accessed October 16, 2021.
- Joint Task Force on Practice Parameters; American Academy of Allergy, Asthma and Immunology; American College of Allergy, Asthma and Immunology; Joint Council of Allergy, Asthma and Immunology. Drug allergy: an updated practice parameter. Ann Allergy Asthma Immunol. 2010;105:259-273.
- McNeil BD. MRGPRX2 and adverse drug reactions. Front Immunol. 2021;12:676354. doi: 10.3389/fimmu.2021.676354.
- Ryder SA, Waldmann C. Anaphylaxis. Contin Educ Anaesth Crit Care Pain. 2004;4:111-113.
- Kemp SF. Pathophysiology of anaphylaxis. UpToDate. Wolters Kluwer; Updated October 11, 2021. www.uptodate.com/contents/pathophysiology-of-anaphylaxis. Accessed February 16, 2022. [Subscription required to access.]
- Bruniera FR, Ferreira FM, Saviolli LRM, et al. The use of vancomycin with its therapeutic and adverse effects: a review. Eur Rev Med Pharmacol Sci. 2015;19:694-700.
- Arroyo-Mercado F, Khudyakov A, Chawla GS, et al. Red man syndrome with oral vancomycin: a case report. Am J Med Case Rep. 2019;7:16-17.
- Pettit NN, DePestel DD, Fohl AL, et al. Risk factors for systemic vancomycin exposure following administration of oral vancomycin for the treatment of Clostridium difficile infection. Pharmacotherapy. 2015;35:119-126.
- Baumgartner LJ, Brown L, Geier C. Hypersensitivity reaction following administration of low-dose oral vancomycin for the treatment of Clostridium difficile in a patient with normal renal function. J Pharm Pract. 2017;30:650-652.
- Barron J, Lattes A, Marcus EL. Rash induced by enteral vancomycin therapy in an older patient in a long-term care ventilator unit: case report and review of the literature. Allergy Asthma Clin Immunol. 2018;14:73. doi: 10.1186/s13223-018-0293-2.
- Bergeron L, Boucher FD. Possible red-man syndrome associated with systemic absorption of oral vancomycin in a child with normal renal function. Ann Pharmacother. 1994;28:581-584.
- Killian AD, Sahai JV, Memish ZA. Red man syndrome after oral vancomycin. Ann Intern Med. 1991;115:410-411.
- Dell Children’s Medical Center of Central Texas. Vancomycin flushing syndrome prevention pathway: pediatric evidence based outcomes center. Updated April 10, 2019. www.dellchildrens.net/wp-content/uploads/sites/60/2019/08/DCMC-Redman-Syndrome-4.10.2019.pdf. Accessed May 18, 2022.
- Renz CL, Thurn JD, Finn HA, et al. Oral antihistamines reduce the side effects from rapid vancomycin infusion. Anesth Analg. 1998;87:681-685.
- Sahai J, Healy DP, Shelton MJ, et al. Comparison of vancomycin- and teicoplanin-induced histamine release and “red man syndrome.” Antimicrob Agents Chemother. 1990;34:765-769.
- Mei H, Wang J, Che H, et al. The clinical efficacy and safety of vancomycin loading dose: a systematic review and meta-analysis. Medicine (Baltimore). 2019;98:e17639. doi: 10.1097/MD.0000000000017639.
- Healy DP, Sahai JV, Fuller SH, Polk RE. Vancomycin-induced histamine release and “red man syndrome”: comparison of 1- and 2-hour infusions. Antimicrob Agents Chemother. 1990;34:550-554.
- Daptomycin. Lexi-Drugs. Lexicomp; Updated May 16, 2022. http://online.lexi.com/. Accessed May 18, 2022. [Subscription required.]
- Telavancin. Lexi-Drugs. Lexicomp; Updated April 19, 2022. http://online.lexi.com/. Accessed May 18, 2022. [Subscription required.]
- Oritavancin. Lexi-Drugs. Lexicomp; Updated April 27, 2022. http://online.lexi.com/. Accessed May 18, 2022. [Subscription required.]
- Dalbavancin. Lexi-Drugs. Lexicomp; Updated April 19, 2022. http://online.lexi.com/. Accessed May 18, 2022. [Subscription required.]
- Svetitsky S, Leibovici L, Paul M. Comparative efficacy and safety of vancomycin versus teicoplanin: systematic review and meta-analysis. Antimicrob Agents Chemother. 2009;53:4069-4079.
- Wazny LD, Daghigh B. Desensitization protocols for vancomycin hypersensitivity. Ann Pharmacother. 2001;35:1458-1464.
- Kitazawa T, Ota Y, Kada N, et al. Successful vancomycin desensitization with a combination of rapid and slow infusion methods. Intern Med. 2006;45:317-321.
- Annè S, Middleton E Jr, Reisman RE. Vancomycin anaphylaxis and successful desensitization. Ann Allergy. 1994;73:402-404.