Receiving chemotherapeutic agents exposes patients with cancer to many complications, including febrile neutropenia. Because of the neutropenic patient’s immune system’s inability to generate an immune response, this complication requires the use of broad-spectrum antibiotics to manage potentially life-threatening infections. Antipseudomonal beta-lactam antibiotics—such as piperacillin-tazobactam, cefepime, or meropenem—are first-line options for the empiric treatment of febrile neutropenia.1 The efficacy for all beta-lactam antibiotics is enhanced when the concentration of the antibiotics is 4- to 5-fold greater than the organism’s minimum inhibitory concentration (MIC).2 To achieve favorable clinical outcomes, penicillins (such as piperacillin-tazobactam) require the time above the MIC to be at least 40% to 50% of the dosing interval.2
Traditionally, piperacillin-tazobactam is given every 6 hours through a standard 30-minute infusion to achieve this time above the MIC.3 An alternative method is to administer piperacillin-tazobactam over an extended period (ie, 4 hours). These extended infusions have been used to achieve increased antibiotic concentrations over a prolonged period, resulting in a longer time above the MIC.3 The attainment of increased antibiotic concentrations and prolonged time above the MIC is necessary for more resistant infectious organisms, including some strains of Pseudomonas aeruginosa, because of the higher MICs observed in these isolates.3-6
Extended infusions use the pharmacodynamics of the antibiotic, allowing for reduced amounts of the drug to be used to attain the goal time above the MIC, thereby potentially decreasing costs and adverse effects, while maximizing efficacy.6 Despite the seemingly apparent benefits of this administration method, there is a paucity of literature to support its use in the high-risk setting of febrile neutropenia. Previous research identified that extended infusions of cefepime for febrile neutropenia have trended toward superiority to intermittent infusions.7,8
A recent study reported a significant increase in overall response with extended infusions of piperacillin-tazobactam or of ceftazidime in patients with febrile neutropenia, while undergoing hematopoietic stem-cell transplantation or induction or consolidation therapy for acute leukemia.9 In other patient populations, meta-analyses of extended infusions in beta-lactam antibiotics have shown benefits regarding mortality and clinical cure.10-14
Based on data that support extended infusions and the growing concern for increasing MICs, St. Vincent Health, Indianapolis, implemented a change in its beta-lactam dosing protocol and implemented extended infusions in 2015. The purpose of this study was to determine the effectiveness of extended infusions of piperacillin-tazobactam in reaching defervescence in the setting of febrile neutropenia.
Methods
The local Institutional Review Board approved this retrospective, single-center study. Adult patients with febrile neutropenia (absolute neutrophil count <500 cells, temperature ≥100.5°F) who were admitted to this community teaching hospital between January 2012 and March 2017, and who were receiving piperacillin-tazobactam, were included in this study. Patients were excluded if defervescence occurred before piperacillin-tazobactam was initiated, or if they received piperacillin-tazobactam after failure of another antipseudomonal beta-lactam antibiotic. If a patient had more than 1 episode of febrile neutropenia during the study period, only the first episode was included in this study.
Data Collection, Identification
The demographic and clinical characteristics that were collected from the electronic health record for all eligible patients included age, length of stay, creatinine clearance, duration of neutropenia, sex, previous chemotherapy, prophylactic antibiotics (ie, quinolone administered prophylactically before onset of febrile neutropenia), mucositis, concomitant vancomycin, granulocyte colony-stimulating factor use, oncologic diagnosis, defervescence, time to defervescence, cost, readmission within 30 days for an infectious condition, inpatient mortality, mortality within 30 days of discharge, microbiologically documented infection, and antibiotic failure.
The moment of defervescence was defined as the time of the first temperature of ≤100.4°F that was sustained for at least 24 hours. Time to defervescence was defined as time from initiation of piperacillin-tazobactam until the moment of defervescence. Antibiotic failure was defined as switching to another antibiotic for any reason other than allergy or intolerance, or inpatient mortality resulting from febrile neutropenia. Cost was calculated by multiplying charges for the hospital stay by the institution’s 2015 ratio of cost to charges.
In addition, Charlson comorbidity score and optimal piperacillin-tazobactam dosing based on the patient’s renal function were determined for each patient. Optimal renal dosing was defined as administration of piperacillin-tazobactam 4.5 g every 6 hours for a creatinine clearance of ≥20 mL/min, piperacillin-tazobactam 4.5 g every 8 hours for a creatinine clearance of <20 mL/min, or undergoing dialysis. Doses outside of these recommendations were considered inappropriate.
The patients were divided into 2 groups—those receiving intermittent infusions and those receiving extended infusions of piperacillin-tazobactam. The intermittent infusions of piperacillin-tazobactam were infused over 30 minutes, whereas the extended infusions were given over 4 hours. Patients receiving extended infusions received their first dose of piperacillin-tazobactam over 30 minutes as a loading dose to ensure the attainment of time above the MIC.
Outcome Measures
The study’s primary outcome measure was defervescence within 24 hours of piperacillin-tazobactam administration. Secondary outcome measures included time to defervescence, antibiotic failure, inpatient and 30-day mortality (ie, 30 days from the start of piperacillin-tazobactam), hospital readmission for an infectious condition, and direct variable cost of hospital admission.
Statistical Analysis
We compared categorical variables between groups using the Fisher exact test or the Pearson chi-square test, as appropriate. We compared continuous variables using the Student’s t-test for parametric data and Mann-Whitney U tests for nonparametric data. We performed binary logistic regression to determine the odds ratios (ORs) of predictors of defervescence at 24 hours (optimal renal dosing, Charlson comorbidity score, prophylactic antibiotics, concomitant vancomycin use, extended infusion, and oncologic diagnosis).
The time to defervescence was analyzed using Kaplan-Meier and Cox regression survival analysis (optimal renal dosing, Charlson comorbidity score, prophylactic antibiotics, concomitant vancomycin use, extended infusion, and oncologic diagnosis). All analyses were performed with Statistical Package for the Social Sciences version 24.0; Chicago, IL. A P value <.05 was considered significant.
Results
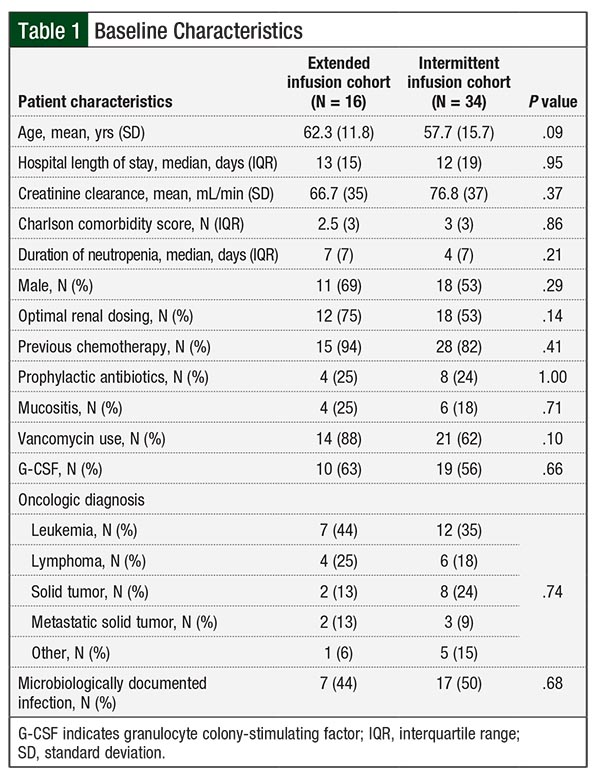
A total of 50 patients were included in the study, 16 of whom received extended infusions (ie, over 4 hours) of piperacillin-tazobactam, and the remaining 34 patients received intermittent infusions. Baseline characteristics were not statistically different between those receiving extended infusions and those receiving intermittent infusions. Of note, 20 patients—4 in the extended infusions and 16 in the intermittent infusions groups—received inappropriate piperacillin-tazobactam dosing and the rate of vancomycin treatment use was 88% in those receiving extended infusions and 62% in those receiving intermittent infusions.
Of the 4 patients in the extended infusions group who received inappropriate dosing, 4 received doses that were too low and 1 of the 4 also received doses at an inappropriate dosing interval. Of the 16 patients in the intermittent infusions group who received inappropriate dosing, 14 received doses that were too low and 4 of them also received doses at an inappropriate dosing interval. Further baseline characteristics are shown in Table 1.
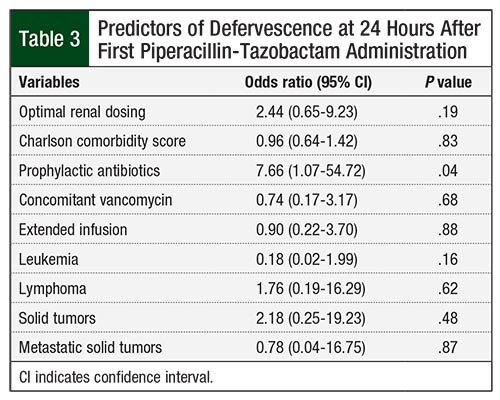
Defervescence at 24 hours—the primary outcome of this study—was similar between the groups (50% in the extended infusions group vs 53% in the intermittent infusions group; P = .85). Logistic regression analysis indicated that extended infusions were not a predictor of defervescence at 24 hours (OR, 0.90; 95% confidence interval [CI], 0.22-3.70; P = .88). The median time to defervescence was also similar between groups (20.8 hours vs 22.8 hours, respectively; P = .84).
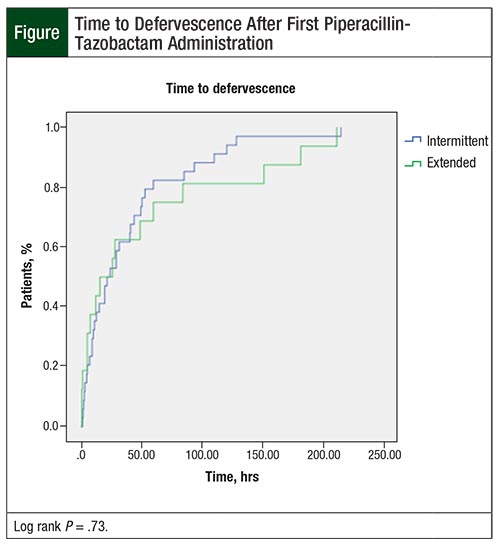
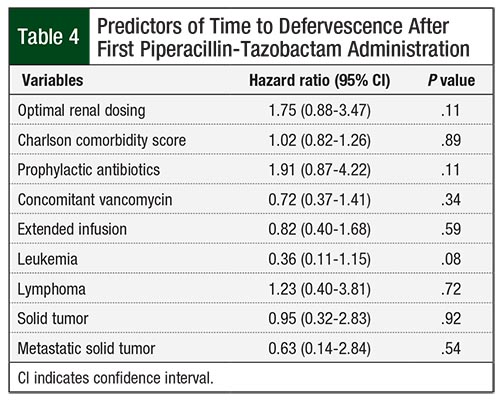
A logistic regression analysis demonstrated that extended infusions were not a predictor of time to defervescence (hazard ratio, 0.82; 95% CI, 0.40-1.68; P = .59). A Kaplan-Meier survival analysis of time to defervescence comparing extended versus intermittent infusions was not statistically significant (Figure; log-rank P = .73).
Both groups had low rates of readmission for an infectious condition within 30 days (0% in the extended infusions group vs 3% in the intermittent infusions group; P = 1.00) and mortality within 30 days (0% vs 6%, respectively; P = 1.00). In addition, the groups had similar rates of antibiotic failure (25% vs 29%, respectively; P = 1.00), inpatient mortality (6% vs 21%, respectively; P = .41), and cost ($23,713 vs $17,116, respectively; P = .53).
A binary logistic regression analysis revealed that receiving prophylactic antibiotics was the only factor that increased the odds of defervescence at 24 hours by 7.66 (95% CI, 1.07-54.72; P = .04). Additional univariate outcomes are displayed in Table 2 and multivariate outcomes are shown in Table 3 and Table 4.

Discussion
Compared with intermittent infusions, extended infusions did not improve outcomes for patients with febrile neutropenia in this study. The only statistically significant difference between the groups was the finding that patients who received prophylactic antibiotics were more likely to defervesce at 24 hours.
In our clinical experience, febrile neutropenia has been managed typically with intermittent infusions (ie, over 30 minutes) of beta-lactam antibiotics, including piperacillin-tazobactam. Using extended infusions of beta-lactam antibiotics helps to optimize drug concentrations, and may serve as a possible response to the ever-present threat of bacterial resistance. Extended infusions allow the beta-lactam antibiotic to maintain an adequate concentration over the MIC; however, there is a lack of studies regarding extended infusions in febrile neutropenia, and although some data with nonneutropenic patient populations are positive, conflicting data exist.
To date, 3 meta-analyses of extended and/or continuous infusions with piperacillin-tazobactam have been published.10,11,14 In a population of patients with pneumonia, sepsis, complicated intra-abdominal infections, and intensive care unit infections, Yang and colleagues reported that extended or continuous infusions of piperacillin-tazobactam almost doubled the odds of clinical cure and lowered the mortality rate by approximately 30%.10
In a subgroup of patients who received piperacillin-tazobactam in the meta-analysis by Falagas and colleagues of continuous and extended infusions of piperacillin-tazobactam or carbapenems, extended infusions of piperacillin-tazobactam decreased the rate of mortality by 45%, but did not demonstrate difference in clinical cure.11
Furthermore, Tamma and colleagues found no difference in mortality or in clinical cure with piperacillin-tazobactam after a subgroup analysis of a meta-analysis of randomized controlled trials of extended or continuous infusion of beta-lactam antibiotics.14 These contradictory outcomes indicate the need to further investigate the place in therapy for extended infusions of piperacillin and tazobactam, particularly in patients with febrile neutropenia.
Recently, a prospective study by Wrenn and colleagues compared extended and intermittent infusions of cefepime for the treatment of febrile neutropenia in patients with a creatinine clearance of ≥50 mL/min.7 Similar rates of defervescence occurred at 24, 48, and 72 hours after starting cefepime; however, there was a trend toward significance, with 17% absolute difference at 24 hours favoring the extended infusion group.7 The time to defervescence also trended toward significance: patients defervesced approximately 22 hours more quickly in the extended infusion arm than in the intermittent infusion arm; however, patients had lower Charlson comorbidity score in the extended infusion arm. Extended infusions also led to similar rates of clinical success, mortality, and length of stay.7
A recent retrospective study of patients with febrile neutropenia also evaluated the use of extended infusions of cefepime; however, it did not exclude patients based on creatinine clearance.8 This study demonstrated that patients receiving extended infusions were more likely to defervesce at 24 hours, and time to defervescence was decreased by 14 hours. Upon multivariate analysis, extended infusions of cefepime quadrupled the odds of defervescence at 24 hours while also doubling the likelihood of defervescence at any time.8
Finally, a prospective randomized clinical trial compared the use of intermittent and extended infusions of piperacillin-tazobactam versus ceftazidime in patients with febrile neutropenia who were undergoing hematopoietic stem-cell transplantation or receiving induction or consolidation therapy for acute leukemia.9 The results demonstrated a significant increase in overall response with extended infusions in the intention-to-treat population; however, no differences were found in fever duration, length of hospital stay, or 30-day mortality. The overall response in the study was defined as the combination of the resolution of fever for at least 24 hours with the use of antibiotics, microbiological eradication (if applicable) on days 3 and 4, resolution of signs and symptoms of infection, and no need for a change in the antibiotic regimen.9
Our study did not show any difference with regard to defervescence at 24, 48, or 72 hours, or time to defervescence. Furthermore, a multivariate analysis showed that extended infusion was not a predictor for either defervescence at 24 hours or time to defervescence. Our study differs from the previously reported study of piperacillin-tazobactam versus ceftazidime for the treatment of febrile neutropenia9 in many ways, including the inclusion of a broader group of oncology diagnoses (leukemia, lymphoma, and solid tumors) and the inclusion of patients with renal dysfunction (ie, patients with creatinine clearance of <40 mL/min excluded from the previous study9).
The population included in our study more closely replicates the general oncology population; it is unknown whether significant benefit would have been found if only patients with leukemia were included. In addition, in the per-protocol analysis of the previous piperacillin-tazobactam study, statistical significance in the primary outcome (ie, overall response) did not exist. Similarly, the duration of fever was similar in both groups in the previous study.9
Prophylactic antibiotics increased the odds of defervescence at 24 hours by 7.66 (95% CI, 1.07-54.72; P = .04) in our study. The exact mechanism of this is unknown, but prophylactic antibiotics may have either selected for pathogens that were susceptible to piperacillin and tazobactam, such as Streptococcus viridans, or decreased the microbiological burden in patients, allowing piperacillin-tazobactam to act more rapidly, leading to earlier defervescence.
Prophylactic antibiotics were used in 24% of the population in our study, whereas 56% of the population in the previous piperacillin-tazobactam versus ceftazidime extended infusion study received prophylactic fluoroquinolones.9 The incidence of microbiologically documented infection was also different between the 2 studies—48% in our study versus 17% in the previous study.9 Secondary outcomes were also similar between the 2 studies—in particular, antibiotic failure, length of hospital stay, and mortality within 30 days.
Despite any significant differences, our findings indicate that the use of extended infusions of piperacillin-tazobactam is a viable option for the treatment of febrile neutropenia; however, extending infusions for more than 4 hours monopolizes the use of an intravenous (IV) access site for a total of 16 hours daily, which may pose administration challenges when patients require administration of other IV medications.
Limitations
The limitations of our study include its retrospective nature and small sample size and limited power. Despite the retrospective nature of our study, the baseline characteristics were similar between the 2 groups (ie, extended vs intermittent infusions). In addition, 40% of the patients did not receive optimal renal dosing according to the definition used in our study, which may prevent the application of this study in other institutions.
However, the previous study of piperacillin-tazobactam versus ceftazidime extended infusions used a piperacillin-tazobactam dose of 4.5 g every 8 hours,9 which was lower than the defined appropriate dose in our study (ie, 4.5 g every 6 hours if creatinine clearance is ≥20 mL/min, or 4.5 g every 8 hours if creatinine clearance is <20 mL/min).
Of note, a pharmacokinetic modeling analysis and Monte Carlo simulation of piperacillin-tazobactam dosing in patients with febrile neutropenia demonstrated that although similar, more frequent dosing (ie, 4 g every 6 hours as an extended infusion compared with 4 g every 8 hours as an extended infusion) may increase the likelihood of attaining time above the MIC for 50% of the dosing interval in patients with higher bacterial MICs (ie, 8 mg/L-16 mg/L) and higher creatinine clearances (ie, >100 mL/min).15
It is unknown whether using a dose of 4.5 g every 6 hours in more patients in our study would have affected the outcomes, especially given the number (48%) of microbiologically documented infections.
Finally, our study also included all patients with febrile neutropenia. It is possible that a subpopulation of patients with febrile neutropenia, such as patients at increased risk for resistant gram-negative infections, may benefit from extended antibiotic infusions.
Conclusion
Febrile neutropenia is an oncologic emergency that requires swift intervention with broad spectrum beta-lactam antibiotics. Previous studies in other patient populations suggest that extending the time of the infusion improves outcomes, but this has not been well-studied in the setting of febrile neutropenia. Optimizing antibiotic therapy especially in a patient population prone to resistant organisms, is vital to improving clinical outcomes. The findings of this study suggest that extended infusions of piperacillin-tazobactam lead to outcomes comparable to intermittent infusions. Further prospective studies in the general oncology population are required to confirm these findings.
Author Disclosure Statement
Dr Przybylski and Dr Reeves have no conflicts of interest to report.
References
- Freifeld AG, Bow EJ, Sepkowitz KA, et al; for the Infectious Diseases Society of America. Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the Infectious Diseases Society of America. Clin Infect Dis. 2011;52:e56-e93.
- Craig WA. Pharmacokinetic/pharmacodynamic parameters: rationale for antibacterial dosing of mice and men. Clin Infect Dis. 1998;26:1-10; quiz 11-12.
- Shea KM, Cheatham SC, Wack MF, et al. Steady-state pharmacokinetics and pharmacodynamics of piperacillin/tazobactam administered by prolonged infusion in hospitalised patients. Int J Antimicrob Agents. 2009;34:429-433.
- Jaruratanasirikul S, Limapichat T, Jullangkoon M, et al. Pharmacodynamics of meropenem in critically ill patients with febrile neutropenia and bacteraemia. Int J Antimicrob Agents. 2011;38:231-236.
- Theuretzbacher U. Pharmacokinetic and pharmacodynamic issues for antimicrobial therapy in patients with cancer. Clin Infect Dis. 2012;54:1785-1792.
- MacGowan A. Revisiting beta-lactams - PK/PD improves dosing of old antibiotics. Curr Opin Pharmacol. 2011;11:470-476.
- Wrenn RH, Cluck DB, Kennedy L, et al. Extended infusion compared to standard infusion cefepime as empiric treatment of febrile neutropenia. J Oncol Pharm Pract. 2018;24:170-175.
- Przybylski DJ, Reeves DJ. Extended versus intermittent infusions of cefepime for the treatment of febrile neutropenia. Infect Dis Clin Pract (Baltim Md). 2018;26:154-158.
- Ram R, Halavy Y, Amit O, et al. Extended vs bolus infusion of broad-spectrum β-lactams for febrile neutropenia: an unblinded, randomized trial. Clin Infect Dis. 2018;67:1153-1160. Erratum in: Clin Infect Dis. 2018;67:1151.
- Yang H, Zhang C, Zhou Q, et al. Clinical outcomes with alternative dosing strategies for piperacillin/tazobactam: a systematic review and meta-analysis. PLoS One. 2015;10:e0116769. doi.org/10.1371/journal.pone.0116769.
- Falagas ME, Tansarli GS, Ikawa K, Vardakas KZ. Clinical outcomes with extended or continuous versus short-term intravenous infusion of carbapenems and piperacillin/tazobactam: a systematic review and meta-analysis. Clin Infect Dis. 2013;56:272-282.
- Teo J, Liew Y, Lee W, Kwa AL. Prolonged infusion versus intermittent boluses of β-lactam antibiotics for treatment of acute infections: a meta-analysis. Int J Antimicrob Agents. 2014;43:403-411.
- Lal A, Jaoude P, El-Solh AA. Prolonged versus intermittent infusion of β-lactams for the treatment of nosocomial pneumonia: a meta-analysis. Infect Chemother. 2016;48:81-90.
- Tamma PD, Putcha N, Suh YD, et al. Does prolonged β-lactam infusions improve clinical outcomes compared to intermittent infusions? A meta-analysis and systematic review of randomized, controlled trials. BMC Infect Dis. 2011;11:181.
- Sime FB, Hahn U, Warner MS, et al. Using population pharmacokinetic modeling and Monte Carlo simulations to determine whether standard doses of piperacillin in piperacillin-tazobactam regimens are adequate for the management of febrile neutropenia. Antimicrob Agents Chemother. 2017;61:e00311-17.