The European Society for Medical Oncology-European Oncology Nursing Society (ESMO-EONS) defines extravasation as the unintended leakage of a substance into the subcutaneous or subdermal tissue around the intravenous or intra-arterial administration site.1 Extravasated drugs are classified as vesicants, irritants, or nonvesicants, according to their potential for causing damage. Vesicants may result in blistering and ulceration, which can lead to tissue destruction and necrosis.1 Irritants have the potential to cause local inflammation, including burning, swelling, pain, tightness, or phlebitis at the infusion site.2 The differential diagnosis of extravasation includes chemical phlebitis, a type of venous inflammation, frequently followed by thrombosis or sclerosis of the veins.1 The common symptoms of any form of phlebitis are erythema and swelling along the venous track, leading to hardened, cordlike veins.3
In 2008, the US Food and Drug Administration (FDA) approved bendamustine (Treanda) for chronic lymphocytic leukemia and indolent B-cell non-Hodgkin lymphoma. Bendamustine was initially prepared at a concentration of 0.2-0.7 mg/mL for injection (45 mg/0.5 mL or 180 mg/2 mL solution) and at a concentration of 0.2-0.6 mg/mL for injection (25 mg per vial of 100 mg per vial lyophilized powder) to be administered as an intravenous infusion for 30 minutes for chronic lymphocytic leukemia indication and 60 minutes for indolent B-cell non-Hodgkin lymphoma.4 With no reports of extravasation injuries in early clinical trials, the original prescribing information for bendamustine did not classify it as an irritant or vesicant. However, postmarketing reports documented extravasation with erythema, marked swelling, and pain that resulted in increased incidence of phlebitis, as well as hospitalizations.4
Bendamustine is identified as an irritant with vesicantlike properties in various drug resources.5 It is classified as an irritant in some literature and as a vesicant in the ESMO-EONS 2012 guideline.1,2
In 2015, the FDA approved a new formulation of bendamustine (Bendeka). This new formulation is prepared to a final concentration of 1.85 to 5.6 mg/mL and administered as an intravenous infusion over 10 minutes.6,7 Although the molecular component of this drug (bendamustine hydrochloride) is the same in the 2 formulations, the new formulation has a higher concentration and a faster administration time than the old formulation.
Although the prescribing information (previous and current versions) for the new formulation of bendamustine contains some details about skin reactions during clinical trials, as well as postmarketing reports of extravasation,7,8 this information seems to have been extrapolated from the old formulation of bendamustine prescribing information, because the adverse events information and data in Table 1 and Table 3 of the prescribing information of both formulations are the same4; there is no evidence in the literature of postmarketing experience with the new formulation of bendamustine in December 2015 when the prescribing information was published.7 As a newly approved formulation, there is still limited postmarketing experience with the new formulation of bendamustine.8
Although postmarketing reports of the old bendamustine extravasation and skin reactions exist in the literature,9 to the best of our knowledge there are no case reports that describe the nature and management of extravasation and skin-related reactions associated with the new formulation of bendamustine.8 We present 2 unique patient cases of bendamustine extravasation or phlebitis, including the case descriptions, management, and follow-up.
Patient Case 1
A 71-year-old woman was diagnosed with stage IV low-grade follicular lymphoma with multiple extranodal disease sites in September 2016. Her relevant medical history included colon cancer (diagnosed in 1990), which was treated with colon resection, and 1 year of adjuvant chemotherapy (5-fluorouracil and levamisole). In October 2016, the patient started treatment with the new formulation of bendamustine 90 mg/m2 on days 1 and 2, and rituximab 375 mg/m2 on day 1 every 28 days.
Bendamustine was given first, followed by rituximab during all treatment cycles. Bendamustine was administered for 10 minutes, according to the prescribing information for all treatment cycles,7 and rituximab was administered after initial infusion rate at cycle 1, noninitial infusion rate at cycle 2, rapid infusion rate at cycle 3, and subsequent cycles according to its prescribing information.10
On cycle 1 of day 1, both medications were administered through a peripheral intravenous line inserted into the patient’s left forearm. The left forearm peripheral intravenous line was used on cycle 1 of day 2, and no redness, pain, or swelling were observed at the intravenous site on day 2. The patient was seen by her oncologist during cycle 1 of day 21, when she reported pain on her left forearm from the previous intravenous site. Her oncologist observed and documented left forearm indentation along the venous track, with a hardened cordlike vein consistent with chemical phlebitis.
On cycle 2 of day 1, bendamustine and rituximab were administered through a peripheral intravenous line inserted into the patient’s right forearm. On day 2, she complained of pain without swelling or redness on the vein of the right forearm used for injection on cycle 2 of day 1. The vein in the right forearm was hardened and cordlike along the venous track, without indentation, while the left forearm from the previous intravenous site of cycle 1 remained hardened and cordlike, with indentation along the venous track. These veins remained painful with bruising at cycle 3 of day 1. Cycle 3 of day 2 was held until a port-a-cath was placed 2 weeks later for administration of subsequent cycles.
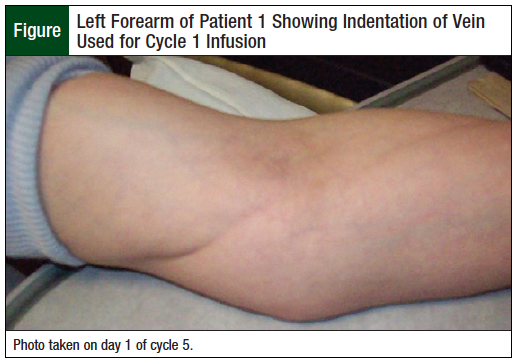
At cycles 4 and 5, the vein in the left forearm from the previous intravenous site of cycle 1 remained painful with hardened, cordlike venous track indentation (Figure), and the vein in the right arm used in cycle 2 remained hardened and cordlike, without indentation and pain.
At cycle 6, the pain in the left vein was resolved; however, it remained mildly indented with a persistent hardened cordlike feel along the venous track, whereas the hardened cordlike sensation on the right venous track was less noticeable. The patient self-reported use of over-the-counter pain medication to alleviate the pain from the affected veins in days 1 and 2 of cycles 1 to 3.
Patient Case 2
A 70-year-old woman was first diagnosed with stage IV follicular lymphoma in 2005 and was treated with rituximab, fludarabine, mitoxantrone, and dexamethasone for 6 cycles, resulting in a complete remission. Subsequently, in 2010, the patient received rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) for 3 cycles for generalized lymphadenopathy. In 2012, the patient was diagnosed with diffuse large B-cell lymphoma and received 3 cycles of the R-CHOP regimen, followed by an autologous stem-cell transplant with a conditioning regimen of rituximab, carmustine, etoposide, cytarabine, and melphalan.
In August 2016, the patient was diagnosed with relapsed follicular lymphoma and started treatment with the new formulation of bendamustine (Bendeka) 90 mg/m2 on days 1 and 2, and rituximab 375 mg/m2 on day 1 of every 28-day cycle. Bendamustine was administered for 10 minutes according to the bendamustine prescribing instructions for all treatment cycles,7 and rituximab was administered after initial infusion rate at cycle 1, and rapid infusion rate at cycle 2, and in subsequent cycles, according to rituximab’s prescribing instructions.10
The patient reported persistent pain and burning from the peripheral intravenous site on the right forearm that was used for cycle 3 during her oncology visit on day 24 of cycle 3. On day 22 of cycle 4, her oncologist observed and documented pain on the left forearm from the cycle 4 peripheral intravenous site. Similar pain and burning sensation was noted and documented at cycle 5. Cycle 6 was held because of low absolute neutrophil count. The pain and burning along the venous track was persistent at 6 months after the patient received treatment at cycle 3.
Discussion
The Visual Infusion Phlebitis score is a valid and reliable phlebitis assessment scale that uses specific skin-related characteristics to describe phlebitis at various stages, ranging from 0 (ie, no signs of phlebitis) to 6 (advanced stage of thrombophlebitis) and provides recommendation for cannula replacement, as well as when to initiate treatment of phlebitis.11 According to this scale, the patient in case 1 is classified as advanced stage of phlebitis (score of 5 points), whereas the patient in case 2 is classified as medium stage of phlebitis (score of 4 points).11
For both patients, the association between bendamustine (Bendeka) and the reported phlebitis is considered a definite adverse drug reaction with a score of 9 based on the Naranjo Adverse Drug Reaction Probability Scale.12 Although both patients were older than age 70 years and had received previous treatment with chemotherapy for previous malignancies, we cannot confidently associate the incidence of phlebitis and skin reaction to their past medical history.
Factors such as pH and osmolarity have previously been identified to have a significant impact on the incidence of chemical phlebitis.13,14
The new formulation of bendamustine has a 9-fold increase in the concentration8 compared with the old formulation of bendamustine.4 We strongly suspect that the increased concentration of the new bendamustine formulation is associated with an increased risk for chemical phlebitis.
The recommendation for all types of phlebitis is to stop the infusion and remove and reinsert the cannula into a different vein, depending on the need and hemodynamic stability of the patient.3,15 Direct application of anti-inflammatory cream or gel to the affected area, as well as oral anti-inflammatory analgesics, have also been documented to minimize the inflammation and treat the pain associated with phlebitis.3,16
Bendamustine is an alkylating agent for which sodium thiosulfate is recommended to manage its extravasation in the same manner as mechlorethamine extravasation.2,17 In the event of bendamustine extravasation, the infusion should be immediately stopped and disconnected, while leaving the cannula/needle in place. The solution should be gently aspirated without flushing the line. The needle/cannula should be removed and the extremity elevated. A dry, cold compress should be applied for 20 minutes 4 times daily.1,2,5 Sodium thiosulfate 1/6 M solution should be injected subcutaneously into the extravasation area using 2 mL for each milligram of the drug suspected to have extravasated.1,18
In our 2 cases of phlebitis, the recommendation for cannula removal and reinsertion was followed as part of routine clinical practice, because the incidence of phlebitis did not occur immediately during the bendamustine infusion but was reported several days after the completion of the bendamustine infusion.
Although the patient in case 1 self-reported the use of over-the-counter pain medication, the specific medication and dose, as well as the effect of pain relief, were not documented. Because both cases are consistent with phlebitis more than extravasation, an appropriate intervention would have been the use of topical and/or oral anti-inflammatory drugs. However, there was no documentation of such prescriptions in the 2 patient cases.
Conclusion
We have observed 2 incidences of phlebitis, indentation, burning, and hardened cordlike feel along the venous track that persisted for 4 to 6 months in patients who received the new formulation of bendamustine using a peripheral intravenous site. At our institution, Houston Methodist Hospital, the new formulation of bendamustine has been classified as a vesicant, which is consistent with the ESMO-EONS guideline classification of bendamustine.1
Our institution has created a vesicant extravasation protocol and an order-set for extravasation management using sodium thiosulfate. We have completed physician, pharmacy, and nursing education about the management of phlebitis and extravasation associated with the new formulation of bendamustine to ensure safe administration of the drug at our institution.
Author Disclosure Statement
Dr Ajewole, Dr Edmondson, Dr McLean, and Dr Heyne have no conflicts of interest to report; Dr Rice is on the Speaker’s Bureau of Novartis, a member of the Ad Hoc Board of Pfizer, Consultant for Alexion and Incyte, and is on the Data Safety Monitoring Committee for Apellis.
References
- Pérez Fidalgo JA, Fabregat LG, Cervantes A, et al. Management of chemotherapy extravasation: ESMO-EONS Clinical Practice Guidelines. Ann Oncol. 2012;23:vii167-vii173.
- Kreidieh FY, Moukadem HA, El Saghir NS. Overview, prevention and management of chemotherapy extravasation. World J Clin Oncol. 2016;7:87-97.
- Higginson R, Parry A. Phlebitis: treatment, care and prevention. Nurs Times. 2011;107:18-21.
- Treanda (bendamustine hydrochloride) injection, for intravenous use [prescribing information]. North Wales, PA: Teva Pharmaceuticals; December 2017.
- Lexi-Comp. Lexicomp Online. Bendamustine. http://online.lexi.com. Accessed September 24, 2017.
- Teva Pharmaceuticals. Teva Pharmaceuticals and Eagle Pharmaceuticals announce FDA approval of Bendeka (bendamustine hydrochloride) injection. December 8, 2015. www.tevapharm.com/news/teva_pharmaceuticals_and_eagle_pharmaceuticals_announan_fda_approval_of_bendeka_bendamustine_hydrochloride_injection_12_15.aspx. Accessed September 23, 2017.
- Bendeka (bendamustine hydrochloride) injection, for intravenous use [prescribing information]. North Wales, PA: Teva; December 2015.
- Bendeka (bendamustine hydrochloride) injection, for intravenous use [prescribing information]. North Wales, PA: Teva; July 2018.
- Carilli A, Favis G, Sundharkrishnan L, Hajdenberg J. Severe dermatologic reactions with bendamustine: a case series. Case Rep Oncol. 2014;7:465-470.
- Rituxan (rituximab) injection, for intravenous use [prescribing information]. South San Francisco, CA: Genentech; January 2019.
- Jackson A. Infection control—a battle in vein: infusion phlebitis. Nurs Times. 1998;94:68, 71.
- Naranjo CA, Busto U, Sellers EM, et al. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther. 1981;30:239-245.
- Kuwahara T, Asanami S, Kawauchi Y, Kubo S. Experimental infusion phlebitis: tolerance pH of peripheral vein. J Toxicol Sci. 1999;24:113-121.
- Kuwahara T, Asanami S, Kubo S. Experimental infusion phlebitis: tolerance osmolality of peripheral venous endothelial cells. Nutrition. 1998;14:496-501.
- Webster J, Osborne S, Rickard C, Hall J. Clinically-indicated replacement versus routine replacement of peripheral venous catheters. Cochrane Database Syst Rev. 2010;CD007798.
- dos Reis PE, Silveira RC, Vasques CI, de Carvalho EC. Pharmacological interventions to treat phlebitis, systematic review. J Infus Nurs. 2009;32:74-79.
- Schulmeister L. Extravasation management: clinical update. Semin Oncol Nurs. 2011;27:82-90.
- Schulmeister L. Safe management of chemotherapy: infusion-related complications. In: Mayer DK, ed. Chemotherapy and Biotherapy Guidelines and Recommendations for Practice. 4th ed. Pittsburgh, PA: Oncology Nursing Society; 2014:283-287.